ВВЕДЕНИЕ
Больные ревматоидным артритом имеют широкий профиль коморбидности, при этом среди сопутствующих патологий у них наиболее распространенными и социально значимыми являются сердечно-сосудистые заболевания, выступающие основной причиной летальности [1–3]. Результаты обсервационных исследований свидетельствуют, что у пациентов с ревматоидным артритом имеется двукратное увеличение сердечно-сосудистого риска по сравнению с общей популяцией, а также высокая частота развития сердечной недостаточности (61–87%), инфаркта миокарда (33–96%), инсульта (24–29%) и других серьезных неблагоприятных кардиоваскулярных событий (30–58%) [4–9].
Наличие сопутствующей патологии оказывает значимое влияние на течение и прогноз ревматоидного артрита, развитие осложнений и его исходы. Однако при своевременной диагностике и соблюдении клинических рекомендаций по лечению достаточно часто удается достигнуть целевых показателей в терапии этих коморбидных состояний. Доказано, что качество жизни пациентов с ревматоидным артритом напрямую связано с его ранней диагностикой и своевременным началом терапии [10–12]. Для управления рисками формирования неблагоприятного течения и своевременного лечения ревматоидного артрита при наличии сопутствующих заболеваний создан ряд национальных и международных рекомендаций. В них изложены алгоритмы клинической и инструментальной оценки развития осложнений, предложен ряд шкал и индексов, позволяющий оценить и прогнозировать течение основного заболевания. Вместе с тем продолжается поиск оптимальной комплексной терапии пациентов с ревматоидным артритом, имеющих широкий спектр коморбидной патологии.
Цель исследования – оценить и сравнить профиль коморбидности в группах больных ревматоидным артритом (РА), протекающим с тромбоцитозом и без тромбоцитоза.
МАТЕРИАЛ И МЕТОДЫ
В исследовании приняли участие 240 пациентов с РА в возрасте старше 18 лет, имеющих среднюю и высокую степень активности заболевания. Диагноз РА был установлен согласно критериям Европейской антиревматической лиги (EULAR) и Американской коллегии ревматологов (ACR) от 2010 г. Все участники проходили обследование и лечение на базе СПб ГБУЗ «Клиническая ревматологическая больница № 25» и были разделены на две равные группы: 120 человек с тромбоцитозом (уровень тромбоцитов >450×109), в том числе 82 (68,3%) женщины; 120 человек с нормальным уровнем тромбоцитов, в том числе 86 (71,7%) женщин.
В исследование и дальнейший анализ были включены сведения о половой принадлежности, возрасте пациентов, данные лабораторных обследований: уровни ревматоидного фактора (РФ), антител к циклическому цитруллинированному пептиду (АЦЦП), высокочувствительного С-реактивного белка (вчСРБ), ферритина, интерлейкина 6 (ИЛ-6), тромбопоэтина (ТПО), растворимого р-селектина. Инструментальное обследование заключалось в определении рентгенологической стадии поражения кистей и стоп по Штейнброкеру. Оценка активности заболевания проводилась с использованием шкалы DAS28 (Desease activity score) по скорости оседания эритроцитов (СОЭ) и СРБ. Пациенты, включенные в исследование, получали базисное лечение в виде метотрексата в дозировке 10–25 мг, при необходимости – патогенетическую (глюкокортикостероиды) и симптоматическую (нестероидные противовоспалительные препараты). В ходе исследования выполнялось межгрупповое сравнение частоты коморбидной патологии у пациентов с РА, имеющих нормальный уровень тромбоцитов и тромбоцитоз.
Медиана продолжительности РА у пациентов с тромбоцитозом и лиц с нормальным уровнем тромбоцитов составила 36 мес. Ранняя стадия заболевания была установлена у 13,3% обследованных.
Статистический анализ полученных данных проводился с использованием пакета программного обеспечения Statistica 12.0 (StatSoft Inc).
РЕЗУЛЬТАТЫ
Результаты клинико-лабораторного обследования сравниваемых групп пациентов с РА представлены в таблице 1. Согласно полученным клинико-лабораторным данным, было выявлено, что уровни СОЭ, вчСРБ, ИЛ-6, ферритина, тромбопоэтина, а также медианные значения активности DAS28 по СОЭ и СРБ оказались достоверно выше у пациентов с РА и тромбоцитозом. Значения АЦЦП и растворимого р-селектина значительно превышали пороговые уровни, но не имели достоверных межгрупповых различий.
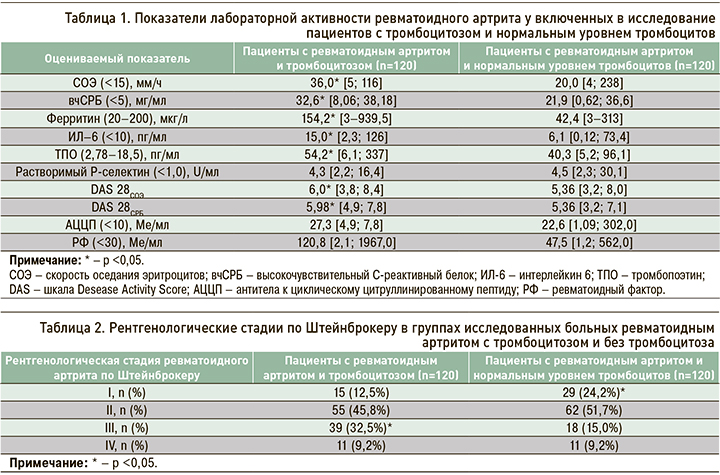
В ходе рентгенографии суставов удалось установить, что у пациентов с РА и тромбоцитозом реже определялась I и чаще устанавливалась III стадия заболевания по Штейнброкеру, чем в группе обследованных с нормальным уровнем тромбоцитов, при одинаковой медианной продолжительности болезни (табл. 2).
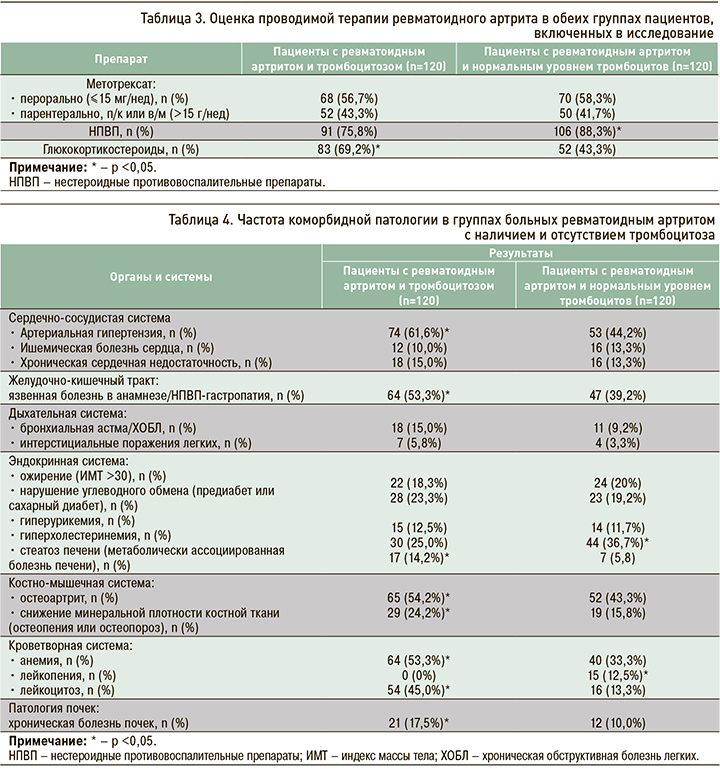
Объяснением столь значимых различий в частоте встречаемости I и III рентгенологических стадий по Штейнброкеру в сравниваемых группах пациентов с РА, скорее всего, служит тот факт, что обследованные с тромбоцитозом имели более агрессивное течение заболевания, способное приводить к быстрому эрозированию суставов. Высокая клинико-лабораторная активность РА требует интенсивного лечения с применением глюкокортикостероидов (ГКС), поэтому на догоспитальном этапе пациентам с уровнем тромбоцитов >450×109 чаще назначались препараты этого класса; в то же время пациенты без тромбоцитоза для купирования болевого синдрома чаще принимали нестероидные противовоспалительные препараты (НПВП) по требованию – 106 (88,3%) случаев против 91 (75,8%) в группе тромбоцитоза (p <0,05; табл. 3). При этом принимаемые дозы метотрексата в обеих группах были сопоставимы.
Известно, что ГКС обладают более значимым противовоспалительным действием, чем НПВП, и, следовательно, могут в большей степени замедлять структурные изменения в суставах. Следует отметить, что в группе обследованных, получавших ГКС, не наблюдались значимые осложнения глюкокортикоидной терапии. В связи с этим можно полагать, что препараты этой группы назначались им согласно клиническим рекомендациям Ассоциации ревматологов России.
Данные различия также могут быть обусловлены наличием сопутствующей коморбидной патологии, при которой прием НПВП противопоказан (язвенная болезнь, кардиоваскулярная и почечная патология и др.). Среди обследованных обеих групп хотя бы одно сопутствующее заболевание встречалось у большинства пациентов (87,5%). Распространенность среди участников исследования различных видов коморбидных состояний по органам и системам представлена в таблице 4.
Исходя из полученных данных, было установлено, что у пациентов с тромбоцитозом из сердечно-сосудистых заболеваний достоверно чаще встречалась артериальная гипертензия, из желудочно-кишечных – язвенная болезнь и/или НПВП-гастропатия, из эндокринных – стеатоз печени, из костно-мышечных – вторичный остеоартрит и снижение минеральной плотности костной ткани согласно критериям Всемирной организации здравоохранения, из болезней кроветворной системы – анемия, в том числе анемия хронического воспаления, и лейкоцитоз (уровень лейкоцитов >9,0×109). Кроме того, у участников исследования с уровнем тромбоцитов >450×109 достоверно чаще определялась хроническая болезнь почек. В свою очередь, у лиц с нормальным уровнем тромбоцитов достоверно чаще выявлялись гиперхолестеринемия и лейкопения (уровень лейкоцитов <4,0×109).
ОБСУЖДЕНИЕ
РА относится к патологиям с широким коморбидным фоном, включающим заболевания сердечно-сосудистой системы и желудочно-кишечного тракта (ЖКТ), а также остеопороз, остеоартрит, сахарный диабет, хронические болезни легких, метаболический синдром и др. [13].
По данным крупного национального исследования США, наиболее частыми причинами госпитализаций пациентов с РА являются сердечно-сосудистые заболевания (около 18%), патологии опорно-двигательного аппарата – вторичный остеоартрит и остеопороз (15%), болезни дыхательной системы (≈12%) и инфекции (≈12%) [14].
Частое развитие сопутствующей патологии при РА, по-видимому, может быть обусловлено несколькими причинами. Так, согласно данным Pope J.E. et al., уровень системного воспаления, интенсивный болевой синдром, длительность утренней скованности и продвинутые рентгенологические стадии РА (III–IV стадии по Штейнброкеру) напрямую коррелируют с кардиоваскулярными заболеваниями, метаболическим синдромом, сахарным диабетом и др. [13]. С другой стороны, немаловажным фактором в развитии сопутствующих заболеваний выступает длительный прием противоревматических препаратов. Известно, что метотрексат может приводить не только к целому ряду нежелательных явлений, связанных с переносимостью этого лекарственного средства, но и участвовать формировании патологии ЖКТ, печени, почек, системы крови и др. Однако следует помнить и о том, что метотрексат обладает способностью снижать частоту сердечно-сосудистых событий у пациентов с РА на 28%.
В соответствии с данными ряда обсервационных исследований, применение преднизолона в дозе >7,5 мг/сут (и в кумулятивной дозе >40 г) было ассоциировано с повышенным риском смертности от всех причин и сердечно-сосудистой смертности независимо от наличия традиционных факторов риска [3]. В то же время в исследовании GLORIA с участием 451 пациента с РА в возрасте 65 лет и старше добавление в комплексную терапию преднизолона в дозе 5 мг/сут в течение 2 лет приводило к снижению показателей активности заболевания и прогрессирования поражения суставов по сравнению с группой плацебо. При этом у пациентов, длительно принимавших этот ГКС, чаще наблюдались нежелательные явления (60 против 49% в группе плацебо), в основном в виде нетяжелых инфекций [15].
Систематический обзор и метаанализ обсервационных исследований и рандомизированных контролируемых исследований выявил повышение риска кардиоваскулярных событий у пациентов с РА на 18% при приеме НПВП. В другом исследовании было показано, что в группе пациентов с РА, получавших НПВП, сердечно-сосудистый риск возрастал на 22% по сравнению с показателями общей популяции. Обращает на себя внимание и тот факт, что длительность терапии НПВП имеет определенные корреляционные связи с развитием патологии ЖКТ, печени, почек и др. [3, 16].
Таким образом, формирование коморбидной патологии при РА является важной проблемой, которая определяется традиционными факторами риска сопутствующих заболеваний, активностью и выраженностью клинических проявлений РА, а также возможными побочными эффектами проводимой медикаментозной терапии. Раннее выявление сопутствующих заболеваний и своевременное их лечение служит важнейшей составляющей комплексной терапии РА.
ЗАКЛЮЧЕНИЕ
В проведенном исследовании было продемонстрировано, что у пациентов с РА и тромбоцитозом имеется более высокая клинико-лабораторная активность основного заболевания в соответствии с показателями СОЭ, СРБ, ферритина, ИЛ-6, индекса DAS 28 и др., а также более значимая рентгенологическая прогрессия болезни, по сравнению с группой больных РА без тромбоцитоза. Такие особенности течения РА требуют более интенсивного лечения, в том числе назначения глюкокортикостероидов в качестве bridge-терапии. Наряду с этим в группе пациентов РА и тромбоцитозом значительно чаще встречается широкий круг коморбидной патологии, что следует учитывать в реальной клинической практике.